Diagnostic codes that really raise suspicion of sepsis
Suspicion of sepsis : Improving the Signal to Noise Ratio
The concept of the SoS paper is reasonable (Inada-Kim M, Page B, Maqsood I, et al Defining and measuring
suspicion of sepsis: an analysis of routine data BMJ Open 2017;7:e014885. doi: 10.1136/bmjopen-2016-014885).
We know that coding of sepsis is poor.
This absence of reliable data makes it hard to compare approaches over time and between locations.
The SoS paper basically lists a lot of codes that the authors associated with infection.
The authors identified 267 codes indicating possible infection.
There were 47475 cases with these codes as a primary diagnosis, with 3440 associated deaths.
We felt that several of these reflected conditions that were not primarily infective in nature
(or at least in which antibiotics would not be a main component of acute management)
We removed the most common of these.
(or at least in which antibiotics would not be a main component of acute management)
We removed the most common of these.
11. N12.X - Tubulo-interstitial nephritis, not specified as acute or chronic
13. J69.0 - Pneumonitis due to food and vomit
54. N10.X - Acute tubulo-interstitial nephritis
62. J84.9 - Interstitial pulmonary disease, unspecified
73. N71.9 - Inflammatory disease of uterus, unspecified
86. K57.1 - Diverticular disease of small intestine without perforation or abscess
90. N48.1 - Balanoposthitis
99. N48.2 - Other inflammatory disorders of penis
130. J69.8 - Pneumonitis due to other solids and liquids
The remaining 258 codes had 45521 cases with 3163 associated deaths.
Figure 1 shows the cumulative frequency of these infection diagnoses ranked by coding frequency.
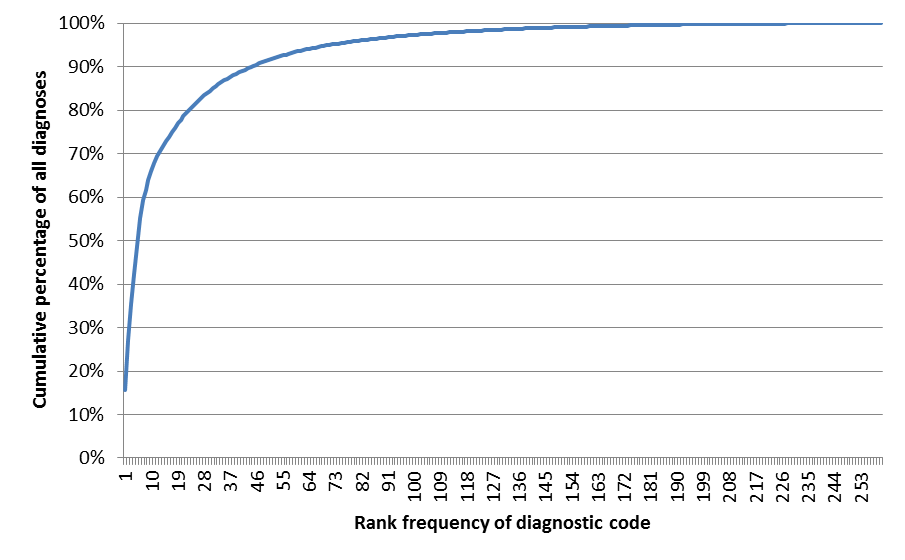
95% of cases are captured using the first 76 diagnostic codes.
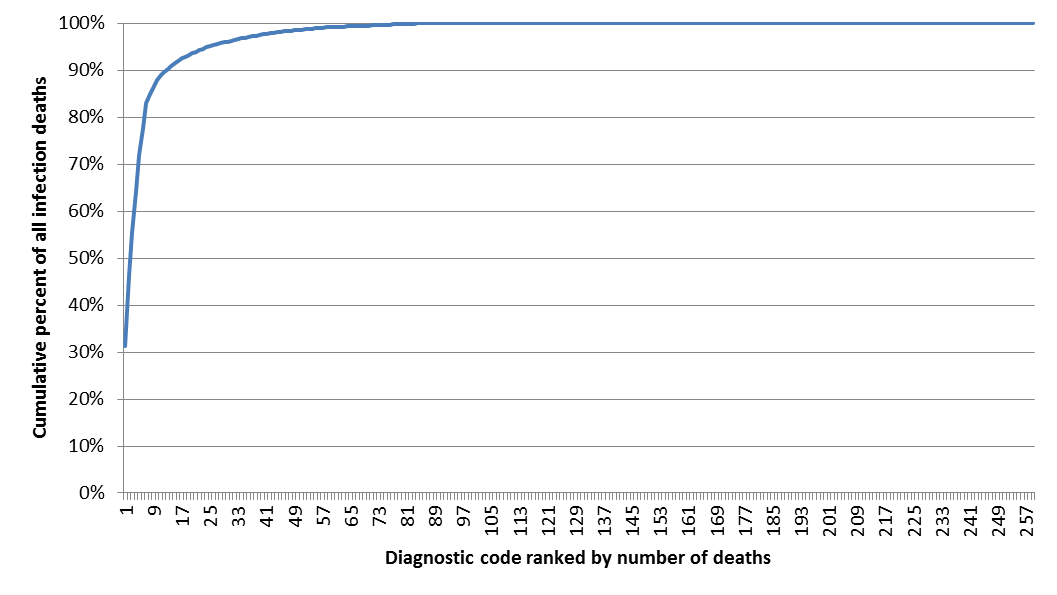
We felt that many of the cases reflected infections that are highly unlikely to progress to death
One would expect this with a condition associated with sepsis.
We ranked the remaining codings by number of deaths.
95% of deaths would be captured in just 24 diagnostic codes.
One would expect this with a condition associated with sepsis.
We ranked the remaining codings by number of deaths.
95% of deaths would be captured in just 24 diagnostic codes.
We added in a number of codes that were highly likely to represent relatively common sepsis conditions,
with mortality over 10% and more than 10 cases.
with mortality over 10% and more than 10 cases.
117. A49.9 - Bacterial infection, unspecified
118. A40.0 - Sepsis due to streptococcus, group A
121. A41.2 - Sepsis due to unspecified staphylococcus
131. A40.3 - Sepsis due to Streptococcus pneumoniae
116. G00.9 - Bacterial meningitis, unspecified
Altogether, these 29 codes accounted for 29424 episodes with 3026 deaths.
We grouped these conditions into overarching infection codes :
Diagnosis
|
admissions
|
deaths
|
Mortality
|
Pneumonia
|
15648
|
2091
|
13%
|
J22.X - Unspecified acute lower respiratory infection
|
3808
|
167
|
4%
|
J18.9 - Pneumonia, unspecified
|
3126
|
483
|
15%
|
J44.0 - COPD with acute lower respiratory infection
|
2854
|
184
|
6%
|
J18.0 - Bronchopneumonia, unspecified
|
432
|
242
|
56%
|
J13.X - Pneumonia due to Streptococcus pneumoniae
|
112
|
11
|
10%
|
J15.1 - Pneumonia due to Pseudomonas
|
51
|
14
|
27%
|
J18.1 - Lobar pneumonia, unspecified
|
5265
|
990
|
19%
|
UTI
|
7088
|
285
|
4%
|
N39.0 - Urinary tract infection, site not specified
|
7088
|
285
|
4%
|
Skin, soft tissue, bone
|
3021
|
73
|
2%
|
L03.1 - Cellulitis of other parts of limb
|
2983
|
62
|
2%
|
M72.6 - Necrotizing fasciitis
|
38
|
11
|
29%
|
Sepsis
|
2615
|
426
|
16%
|
A41.9 - Sepsis, unspecified
|
1882
|
280
|
15%
|
A41.5 - Sepsis due to other Gram-negative organisms
|
360
|
40
|
11%
|
A41.8 - Other specified sepsis
|
87
|
32
|
37%
|
A41.0 - Sepsis due to Staphylococcus aureus
|
70
|
24
|
34%
|
A41.1 - Sepsis due to other specified staphylococcus
|
40
|
9
|
23%
|
A40.8 - Other streptococcal sepsis
|
34
|
6
|
18%
|
J15.0 - Pneumonia due to Klebsiella pneumoniae
|
27
|
8
|
30%
|
A40.9 - Streptococcal sepsis, unspecified
|
21
|
3
|
14%
|
R57.2 - Septic shock
|
21
|
11
|
52%
|
A49.9 - Bacterial infection, unspecified
|
19
|
3
|
16%
|
A41.2 - Sepsis due to unspecified staphylococcus
|
19
|
4
|
21%
|
A40.0 - Sepsis due to streptococcus, group A
|
19
|
4
|
21%
|
A40.3 - Sepsis due to Streptococcus pneumoniae
|
16
|
2
|
13%
|
Abdominal
|
723
|
122
|
17%
|
K57.2 - Diverticular disease of large intestine with perforation and abscess
|
231
|
20
|
9%
|
A04.7 - Enterocolitis due to Clostridium difficile
|
208
|
20
|
10%
|
K63.1 - Perforation of intestine (nontraumatic)
|
136
|
51
|
38%
|
K65.0 - Acute peritonitis
|
96
|
13
|
14%
|
K65.9 - Peritonitis, unspecified
|
52
|
18
|
35%
|
Biliary
|
240
|
18
|
8%
|
K83.0 - Cholangitis
|
240
|
18
|
8%
|
Endocarditis
|
89
|
11
|
12%
|
I33.0 - Acute and subacute infective endocarditis
|
89
|
11
|
12%
|
Grand Total
|
29424
|
3026
|
10%
|
In conclusion, we captured 96% of infection deaths using just 29 diagnostic codes.
It is thus possible to simplify the analysis of Inada Kim et al considerably,
and by so doing improve the signal to noise ratio of the analysis.
We still included some conditions that are not primarily infective (eg abdominal perforation)
However, this led us to consider that a practical definition of sepsis might be
"A diagnosis for which antibiotics would generally be seen as part of acute management"
The paper only looks at primary codes, and this might miss hospital acquired sepsis.
We agree that this is likely to increase noise, but this is an area that merits further research.
We also note that the authors state “although there are non-bacterial causes of sepsis (eg, viruses, protozoa), these are (generally) far less common and amenable to treatment”
Given that influenza is one of the commonest causes of death from infection, this is perhaps hard to justify.
This will help comparative studies of sepsis management,
and provide focus on the areas that are likely to be benefit from attention.
It is thus possible to simplify the analysis of Inada Kim et al considerably,
and by so doing improve the signal to noise ratio of the analysis.
We still included some conditions that are not primarily infective (eg abdominal perforation)
However, this led us to consider that a practical definition of sepsis might be
"A diagnosis for which antibiotics would generally be seen as part of acute management"
The paper only looks at primary codes, and this might miss hospital acquired sepsis.
We agree that this is likely to increase noise, but this is an area that merits further research.
We also note that the authors state “although there are non-bacterial causes of sepsis (eg, viruses, protozoa), these are (generally) far less common and amenable to treatment”
Given that influenza is one of the commonest causes of death from infection, this is perhaps hard to justify.
This will help comparative studies of sepsis management,
and provide focus on the areas that are likely to be benefit from attention.


Comments
Post a Comment